
WHAT IS C-PEPTIDE?
BETA-CELL FUNCTION CAN BE ASSESSED BY MEASURING
C-PEPTIDE1-4
ASSESSING BETA-CELL ACTIVITY BY MEASURING C-PEPTIDE LEVELS CAN HELP IDENTIFY THE EXTENT OF T1D PROGRESSION3
Once a patient is diagnosed, C-peptide testing can identify the extent of beta-cell function1-4
C-PEPTIDE IS THE "GOLD STANDARD" FOR ASSESSING BETA-CELL FUNCTION, ACCORDING TO THE ENDOCRINE SOCIETY6
C-peptide provides a more reliable measure of beta-cell function vs insulin1,7-9
C-PEPTIDE TESTING
There are multiple factors associated with the usefulness of C-peptide testing, including its reliability and options for types of tests1,7-9
C-PEPTIDE
Reliable measure of beta-cell function due to1,7-9:
- Constant rate of clearance
- Not being affected by exogenous insulin
INSULIN
Difficult to measure accurately due to1,7-9:
- Variable rate of clearance
- Being impacted by exogenous insulin
TYPES OF TESTS1,10,11
STIMULATED
Provides the most accurate picture by using a trigger, like a meal or glucagon, to provoke an insulin response
FASTING
Measures baseline production after an overnight fast
RANDOM NON-FASTING
Measures current production without regard to food intake
INTERPRETING C-PEPTIDE MEASUREMENTS FOR BETA-CELL FUNCTION
Since C-peptide and insulin are secreted by beta cells at a 1:1 ratio, remaining beta-cell function can be assessed by measuring C-peptide1-4
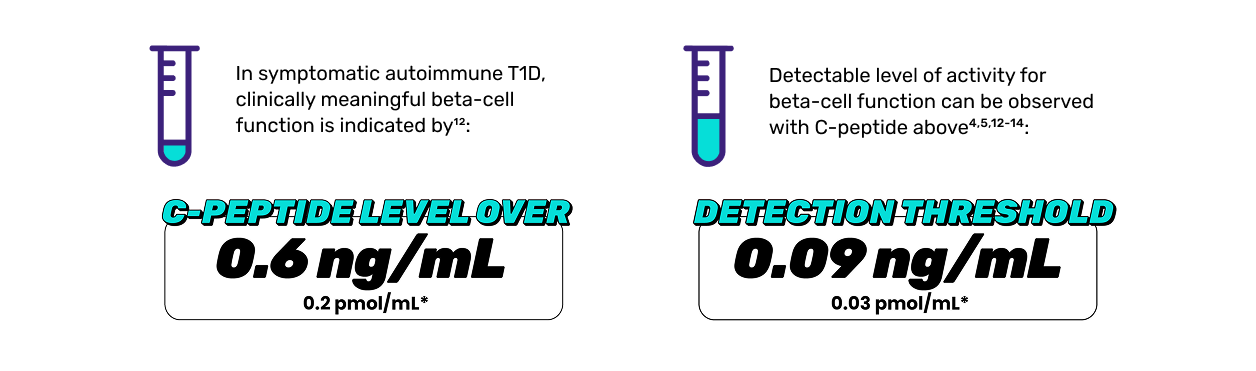
*Based on a conversion from 0.2 pmol/mL using the molecular weight of 3020.3 g/mol for C-peptide.1-4
These codes are provided as examples only and are not all-inclusive; appropriate codes can vary by patient, setting of care, and payer. This information is not meant to provide medical or legal advice or recommendations regarding the use of specific codes for billing purposes. The provider submitting the claim is responsible for determining the medical necessity, appropriate coding, and accuracy of claims.
CPT is the registered trademark of the American Medical Association. Other third-party marks are the property of their respective owners.
*A specific test code may be required in addition to the CPT code. Please confirm which codes are required for your preferred laboratory.
CPT=Current Procedural Terminology.
MEASURING C-PEPTIDE TO ASSESS BETA-CELL FUNCTION IS IMPORTANT FOR THE EVALUATION OF T1D3
References
-
Leighton E, Sainsbury CAR, Jones GC. A practical review of C-peptide testing in diabetes. Diabetes Ther. 2017;8(3):475-487.
-
Palmer JP, Fleming GA, Greenbaum CJ, et al. C-peptide is the appropriate outcome measure for type 1 diabetes clinical trials to preserve β-cell function: report of an ADA workshop, 21-22 October 2001. Diabetes. 2004;53(1):250-264.
-
Pociot F. Capturing residual beta cell function in type 1 diabetes. Diabetologia. 2019;62(1):28-32.
-
Latres E, Greenbaum CJ, Oyaski ML, et al. Evidence for C-peptide as a validated surrogate to predict clinical benefits in trials of disease-modifying therapies for type 1 diabetes. Diabetes. 2024;73(6):823-833.
-
Sørensen JS, Johannesen J, Pociot F, et al; Danish Society for Diabetes in Childhood and Adolescence. Residual β-cell function 3-6 years after onset of type 1 diabetes reduces risk of severe hypoglycemia in children and adolescents. Diabetes Care. 2013;36(11):3454-3459.
-
Michels AW, Brusko TM, Evans-Molina C, et al. Chages and opportunities for understanding the pathogenesis of type 1 diabetes: an Endocrine Society scientific statement. J Clin Endocrinol Metab. 2025;110(9):2496-2508.
-
Maddaloni E, Bolli GB, Frier BM, et al. C-peptide determination in the diagnosis of type of diabetes and its management: a clinical perspective. Diabetes Obes Metab. 2022;24(10):1912-1926.
-
Stankute I, Verkauskiene R, Dobrovolskiene R, et al. Kinetics of C-peptide during mixed meal test and its value for treatment optimization in monogenic diabetes patients. Diabetes Res Clin Pract. 2021;178:108938.
-
Jones AG, Hattersley AT. The clinical utility of C-peptide measurement in the care of patients with diabetes. Diabet Med. 2013;30(7):803-817.
-
Greenbaum CJ, Mandrup-Poulsen T, McGee PF, et al; Type 1 Diabetes Trial Net Research Group; European C-Peptide Trial Study Group. Mixed-meal tolerance test versus glucagon stimulation test for the assessment of β-cell function in therapeutic trials in type 1 diabetes. Diabetes Care. 2008;31(10):1966-1971.
-
Hope SV, Knight BA, Shields BM, et al. Random non‐fasting C–peptide: bringing robust assessment of endogenous insulin secretion to the clinic. Diabet Med. 2016;33(11):1554-1558.
-
Flatt AJS, Greenbaum CJ, Shaw JAM, et al. Pancreatic islet reserve in type 1 diabetes. Ann N Y Acad Sci. 2021;1495(1):40-54.
-
Lachin JM, McGee P, Palmer JP; DCCT/EDIC Research Group. Impact of C-peptide preservation on metabolic and clinical outcomes in the Diabetes Control and Complications Trial. Diabetes. 2014;63(2):739-748.
-
Gubitosi-Klug RA, Braffett BH, Hitt S, et al; DCCT/EDIC Research Group. Residual β cell function in long-term type 1 diabetes associates with reduced incidence of hypoglycemia. J Clin Invest. 2021;131(3):e143011.
MAT-US-2601779-v1.0-03/2026